
CLINICAL CASE
Acute renal failure due to oxalate in a 64-year-old patient
Insuficiencia renal aguda por cristales de oxalato en un paciente de 64 años
María Ajenjo González1, Igor Romaniouk Jakovler2, Natalia Allende3, María del Carmen Barnes4
* Autor para correspondencia.
Correo electrónico: majenjo.g@gmail.com (María Ajenjo González).
![]()
![]()
This work is licensed
under a Creative
Commons
Attribution-NonCommercial-ShareAlike 4.0 International License
La revista no cobra tasas por el envío de trabajos,
Mr. Editor.
Acute renal failure due to oxaluria is a rare entity. Primary hyperoxaluria tends to manifest at an early age and is mainly due to an enzymatic deficit(1,2,3,4). Secondary hyperoxaluria is more common and has multiple causes such as: enteric malabsorption, celiac sprue, pancreatic insufficiency or short bowel syndrome(4); other causes of secondary hyperoxaluria are: a rich oxalate diet, intoxication with ethylene glycol, excessive intake of ascorbic acid and adverse reactions to methoxyfluoran. We present the case of a 64-year-old patient admitted in nephrology due to acute renal failure of unknown etiology, whose renal biopsy revealed a deposit of oxalate crystals(5).
A 64-year-old patient admitted to nephrology in March 2017th at the University Hospital Son Espases due to an acute renal failure. Patient background includes: Tricholeukemia diagnosed and treated in in 1999 in Madrid, episode of acute pancreatitis in 2000nd admitted at University Hospital Puerta del Hierro in Madrid. Diabetes Mellitus type 2 diagnosed in 2006 treated with euglycin. Hyperuricemia with gout episodes, and mild episodes of nephritic colic treated in primary care in Palma de Mallorca.
The initial test reported: a glomerular filtered rate (GFR) of 5 ml/min/1.73 m2, a urea of 190 mg/dl and a creatinine level of 9.96 mg/dl, hemoglobin of 8.8 g/d, 12,000 leucocytes with and 83% of neutrophils, no eosinophilia was observed. The initial urinary exam suggestive of an active infection with no traces of crystals, probably due to an active respiratory and urinary infections secondary to a multi sensitive E. Coli and Chlamidophila pneumoniae treated with antibiotics with negative posterior cultures.
Due to the gravity of the situation the patient begins hemodialysis using a jugular temporal catheter. The patients maintained a 1000 cc diuresis. Abdominal ultrasound: normal-size kidneys with a diffuse increase in echogenicity and probable nephropathy. No hydronephrosis. Normal size liver, presence of hyperechoic millimeter images (left hepatic lobe) compatible with calcifications (calcified granulomas), seen in previous ultrasound in December 2006th.
The autoimmunity study: ANCA positive at low titration with atypical pattern (anca X), Anti-MPO, Anti-PR3 and Anti-MBG negative; Rheumatoid factor <10, C3 and C4 normal. Immunoglobulins: IgG 470, IgA 55, IgM 18. In the absence of evidence of the etiology of renal failure, it was decided to perform a renal biopsy, reporting (Figure 1): 25 Glomeruli presenting 11 of them with some of them with fibrous thickening of the capsule, no images suggestive of light chain glomerulopathy, no evidence spikes, or matrix accumulations, presence of numerous crystals could be observed(6). The history of alcoholism, malabsorption and pancreatitis, gout episodes and mild nephritic colic’s and hyperuricemia led to a suspicion of un underlying kidney affection that hasn’t been found yet.
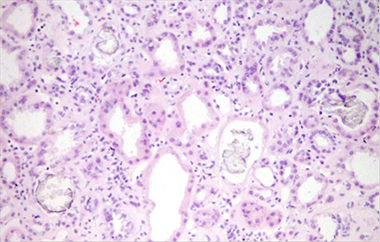
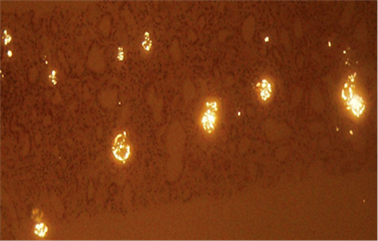
Figure 1. Renal biopsy, a numerous oxalate cristals can be observed.
With this new founding, a 24 hours urine test was done reporting: oxalate in urine 24h (concentration and excretion): and 49.18 mg/L and 83.6 mg/24h. The patient started treatment with volume, and calcium carbonate without any improvement, continuing on hemodialysis which makes us suspect even more damage than initially expected(7).
This clinical case illustrates the consequences of late diagnosis of a not frequent entity. The most common manifestations of hyperoxaluria are the presence of nephrocalcinosis and urolithiasis, especially in early ages(8). In out case, there was no visible renal calcifications eve though some liver calcifications were detected. Some conditions such as the chronic pancreatitis secondary to alcoholism causing a possible malabsorption and subsequent formation of oxalate crystals over the time might explain the acute renal failure secondary to oxalate crystals. The renal biopsy and the was definitive for the diagnosis. Generally, oxalate deposits appear in the terminal phase of renal failure(9), making it hard to detect in earlier stages. Although, acute renal failure by oxalate crystals is not a frequent entity, it may appear in certain patients. In the lack of objective laboratory data, the clinical history is essential as well as its prompt referral to nephrology to avoid further damage(10).
Referencias
1. Víctor L- Sellares, Víctor Lorenzo, Armando T Ramírez, Armando Torres et al. Primary hyperoxaluria. Nefrologia 2014;34:398-412 | doi: 10.3265/Nefrologia.pre2014.Jan.12335
2. Beck BB, Hoppe B. Is there a genotype-phenotype correlation in primary hyperoxaluria type1? Kidney Int. 2006;70:984-6
3. P Cochat, G Rumsby Primary hyperoxaluria N Engl J Med, 369 (2013), pp. 649-658
4. Hoppe B, Beck BB, Milliner DS. The primary hyperoxalurias. Kidney Int 2009;75(12):1264-71.
5. Agrawal V, Liu XJ, Campfield T, et al. Calcium oxalate supersaturation increases early after Roux-en-Y gastric bypass. Surg Obes Relat Dis n n2013; 10: n88-94.
6. Lefaucheur C, Hill GS, Amrein C, Haymann JP, Jacquot C, Glotz D, et al.??Acute oxalate nephropathy: A new etiology for acute renal failure following nonrenal solid organ transplantation. Am J Transplant 2006;6(10):2516-21. Epub 2006 Aug 1.
7. Yamaguchi S, Wiessner JH, Hasegawa AT, Hung LY, Mandel GS, Mandel NS.Study of a rat model for calcium oxalate crystal formation without severe renal damage in selected conditions. Int J Urol. 2005 Mar;12(3):290-8.
8. Trotter JF, Milliner D. Auxiliary Liver Transplant Is an Ineffective Treatment of Primary Hyperoxaluria. Am J Transplant 2014;14(1):24.
9. Marengo SR, Romani AM. Oxalate in renal stone disease: the terminal metabolite that just won't go away. Nat Clin Pract Nephrol 2008;4(7):368-77. Epub 2008 Jun 3.
10. Delayed diagnosis of primary hyperoxaluria in a young patient with advanced chronic renal failure. M. Martín, G. Martín Reyes, A. Torres de Rueda et al, versión On-line ISSN 1989-2284versión impresa ISSN 0211-6995. Nefrología (Madr.) vol.31 no.2 Cantabria 2011.