
ORIGINAL
Lifestyle and clinical factors affecting the quality of life related to health[1]
Estilo de vida y factores clínicos que afectan a la calidad de vida relacionada con la salud
Begoña de Cuevillas1, Santiago Navas-Carretero1, Alejandro Fernández-Montero2, Marta Cuervo1, J. Alfredo Martínez1
1 Department of Nutrition, Food Science, Physiology and Toxicology, Centro de Investigación en Nutrición, Universidad de Navarra, Pamplona, Navarra, Spain.
2 Área de Medicina del Trabajo del Servicio de Prevención de Riesgos Laborales. Clínica Universidad de Navarra, Pamplona, Navarra, Spain.
* Autor para correspondencia.
Correo electrónico: jalfmtz@unav.es (J. Alfredo Martínez).
![]()
![]()
This work is licensed
under a Creative
Commons
Attribution-NonCommercial-ShareAlike 4.0 International License
La revista no cobra tasas por el envío de trabajos,
Abstract
Background. Few studies have examined the influence of personal, phenotypical and lifestyle habits on quality of life related to health.
Methods. Cross-sectional study, which was conducted on 106 patients (63 women). Quality of life was measured by the Short-Form 36 (SF-36) questionnaire while lifestyle factors were evaluated with a general questionnaire developed by the authors of the study, with the Mediterranean Diet Adherence Screener (MEDAS) and with the Global Physical Activity Questionnaire (GPAQ). Participants were divided into two groups (lower and higher global health) attended to their punctuation on the SF-36.
Results. The 8 domains of the SF-36, quantifying the quality of life, were influenced by sex and age. A total of 51 out 106 were qualified as lower global health (score lower than 84.8 points). No significant differences were found how lifestyle factors, body composition and blood biomarkers affect the quality of life between groups. The three dimensions of the SF-36 and the transition of health question were not significantly influenced by any of the items analyzed.
Conclusion. This research enabled us to obtain a pilot vision of the lifestyle of the population and the planning of future research despite that the outcomes were not sufficient satisfactory.
Keywords
lifestyle; quality of life; SF-36
Resumen
Introducción. Los estudios que han examinado la influencia de los hábitos personales, fenotípicos y de estilo de vida en la calidad de vida relacionada con la salud son escasos.
Resultados. Los 8 dominios del cuestionario SF-36 que cuantifican la calidad de vida, se vieron influidos por el sexo y la edad de los participantes. Un total de 51 de los 106 voluntarios se calificaron en el grupo de mejor salud total (puntuación inferior a 84,8 puntos). No se encontraron diferencias significativas entre los grupos en cómo el estilo de vida, la composición corporal y los marcadores bioquímicos afectan la calidad de vida. Las tres dimensiones del cuestionario SF-36 y la pregunta de transición de la salud no se vieron significativamente influenciadas por ninguno de los items analizados.
Conclusión. Este estudio nos permite obtener una visión previa del estilo de vida de la población y para planificar futuras investigaciones a pesar de que los resultados no fueron suficientemente satisfactorios.
What the study adds
This research enabled us to obtain a pilot vision of the lifestyle of the population and the planning of future research lines. This study has allowed to find a relationship between multiple phenotypic factors and lifestyle with quality of life related to health. These results are in accordance with the existing bibliography. However, it has also allowed us to highlight the importance of some factors such as fat mass on quality of life, which is essential due to the lack of existing literature on it.
In summarie, with the results obtained, it would be interesting to continue investigating the effects of some phenotypic factors, such as fat mass, physical activity and other clinical information on the quality of life related to health. On the other hand, due to the current population’s interest to maintain a healthy lifestyle, it would also be of scientific interest to continue investigating on the influence that diverse factors have on the quality of life.
Introduction
Throughout the years, the concept of health has received several definitions because it is a notion that encompasses several factors, which makes it complex and difficult to summarize(1). The most commonly used definition is the one provided by the World Health Organization (WHO), which states health is a status of complete physical, mental and social well-being and not merely the absence of disease or disability(2).
Several studies have shown that certain changes in lifestyle are effective in improving people’s health and reducing the burden of diseases(3). Some authors define “lifestyle” as a general way of living based on the interplay between living conditions in the wide sense and individual patterns of behavior as determined by sociocultural factors and personal characteristics(4). The conditions where people grow, live, work and grow old, greatly influence the way people live and die in the long run(5). Almost half of deaths and most of the diseases that occur every year are mainly due to lifestyle factors. These conditions are circumstances that makes the intervention on lifestyle of the general population a priority issue and of great interest to a public health level(1). The lifestyles of Western countries include many practices or behaviors that can be a risk to health. These most common behaviors are the consumption of tobacco, the consumption of alcohol, an inadequate diet (rich in fats and sugar) and physical inactivity(6).
Despite the importance of lifestyle and the relevance of health in our lives, the measurement of health is somewhat diffuse in the medical literature, while it is an emerging phenomenon(7). In the last years, health has become a social commodity, where citizens have a right and it is perceived as one of the determinants of personal development and the happiness of a person o community(8). The term Quality of Life (QoL) refers to the physical, emotional and social well-being of people, as well as they capacity to get on and develop the typical tasks of daily life. While the concept of QoL includes different aspects of our lives, such as where we live, job satisfaction, etc., Health Related to Quality Of Life (HRQoL) only covers aspects of our lives that are dominated or significantly influenced by personal health and the activities we perform to maintain or improve health(8).
Maybe, the most commonly used questionnaire to measure quality of life is the 36-Item Short-Form Health Survey (SF-36) due to its reliability and validation. The SF-36 provides a profile of the state of health and is one of the most widely used generic scales in the evaluation of clinical outcomes(9). This questionnaire consists of 36 questions, 35 of which evaluate health along 8 dimensions: physical functioning, role limitations due to physical health, role limitations due to emotional problems, vitality, mental health, social functioning, bodily pain and general health(10).
In this context, and due to the current population’s interest to maintain a healthy lifestyle, we examined whether personal, phenotypical and lifestyle factors are associated with quality of life related to nutrition and health.
Methods
The cohort study was established in 2018, based on 106 workers (63 women) of the Clinica Universidad de Navarra (CUN), the Universidad de Navarra (UNAV) or at the Centro de Investigación Médica Aplicada (CIMA) aged 21-66 years old. All participants provided an informed consent.
Outcome
All the questionnaires were administered in one occasion between March to May 2018. The 36-item questionnaire has eight scales: physical functioning, physical role limitation, pain, general health, vitality, social functioning, emotional role limitations and general health perception(10). The scales can be summarized into mental health (MH) and physical health (PH) based on factor analysis to produce two scores scaled from 0 to 100 (high score indicating good health)(11). MH and PH together form global health (GH). We used data to define lower global health as the punctuation lower that 84.8 points to categorize the population according to the median.
Variables
The height, waist circumference and hip circumference were measured with a measuring tape and blood pressure with a sphyngomanometer, by certified staff members following standardized protocol. Participants were also measured for weight, BMI and fat mass by bioimpedance (TBF-410GS, TANITA, Tokyo, Japan) using an appropriate manual. The degree of obesity was calculated based on the BMI (kg/m2).
Physical activity at work and during free time was assessed in minutes according to the validated questionnaire GPAQ, as well as the time of displacement(12). Adherence to the Mediterranean Diet was assessed by combining 12 questions about food consumption frequency (olive oil, vegetables, fruits, meat, saturated lipids and margarines, nonalcoholic beverages, red wine, legumes, fish, commercial pastries, nuts, and sofrito) and 2 more questions on food intake habits characteristic of the Mediterranean Diet (one for use olive oil as the principal source of fat and one for preferring white meat over red meat consumption)(13).
To obtain biochemical data, blood samples were analyzed from each participant following routine protocol at the CUN, which is a certified laboratory. Blood biomarkers were measured using the routine standard on the CUN. Data of the following variables were collected: systolic pressure, diastolic pressure, total cholesterol, HDL cholesterol, LDL cholesterol, creatinine, GGT, glucose, basophils, MCHC, eosinophils, hemoglobin, MCH, red blood cells, hematocrit, leukocytes, lymphocytes, monocytes, neutrophils, PDW, platelets, PCT, RDW, TSH, PCR, triglycerides and urate.
Statistical methods
All analyses were performed using STATA version 12.1 statistical software (StataCorp, College Station, TX). Distribution of variables was assessed through the Shapiro Wilk test. Thus, with those variables following a normal distribution was used parametric statistical test while those variables with a no normal distribution non-parametrical statistics was applied.
Descriptive statistics were used to compare the data of the participants separated by sex and age. For continuous variables student t-test (for parametric) of independent samples and U-Mann Whitney (for non-parametric variables) were applied. Categorical variables were analyzed by using the chi-squared test and were reported as percentage. Then, each dimension of the SF-36 was coded, aggregated and transformed into a scale with a range of 0 to 100. The median was calculated, and the population was categorized according to it, obtaining to groups (n=51 each): the one considered as “Lower Global Health” (52.0-84.8 points) and the other one considered as “Higher Global Health” (84.8-99.0 points).
Once the population was distributed, the descriptive statistical analyses were carried out. Four categories were divided based on age and sex, there were: Men under 40, Women under 40, Men over 40 and Women over 40. Means (SD) were calculated for each variable of the eight domains across categories and assessed statistical significance of the differences among them and interactions with two-way factorial ANOVA (age and sex). In those variables, where there were significant differences between sex and age, a Bonferroni's post-hoc method posteriori was performed. Finally, linear regression models were set up with variables of interest such a BMI, age, physical activity, Diseases Ratio Score (DRS), physical activity at work and sitting time as independent variables and as the three dimensions of the SF-36 (Physical Health, Mental Health, Global Health) and transition of health question as dependent variables. Statistical significance (two-tailed) was established at p < 0.05.
Results
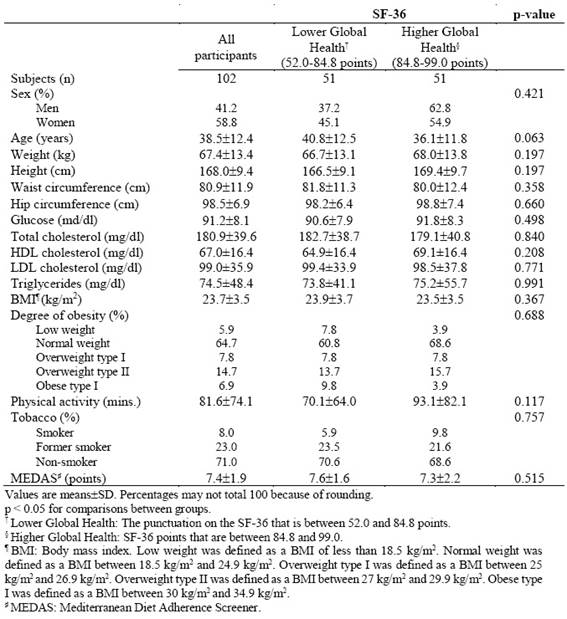
After categorizing the participants according to the score obtained in the SF-36 questionnaire, the volunteers with the highest score shows no significant differences in any of the lifestyle factors comparing to the lower global health group. No significant differences were found in the blood biomarkers and hemogram between the higher and lower global health groups. Also, there were not significant differences in body composition between groups (Table 1).
Table 1. Baseline characteristics, body composition, physical activity, dietary habits and some blood biomarkers of all the participants in the study classifying them by SF-36.
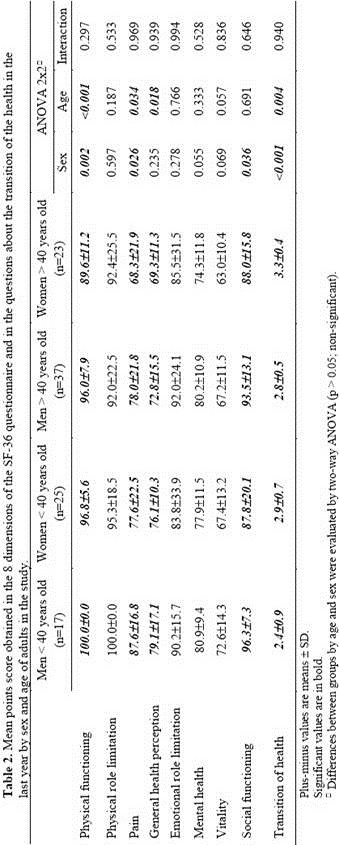
The mean value of physical functioning, pain and transition of health was influenced by the sex and by the age of the participants. However, general health perception depends only on the age variable (p=0.018), and the domain social functioning has only been influenced by sex (p=0.036). However, no interactions between the variables were featured in any case (Table 2).
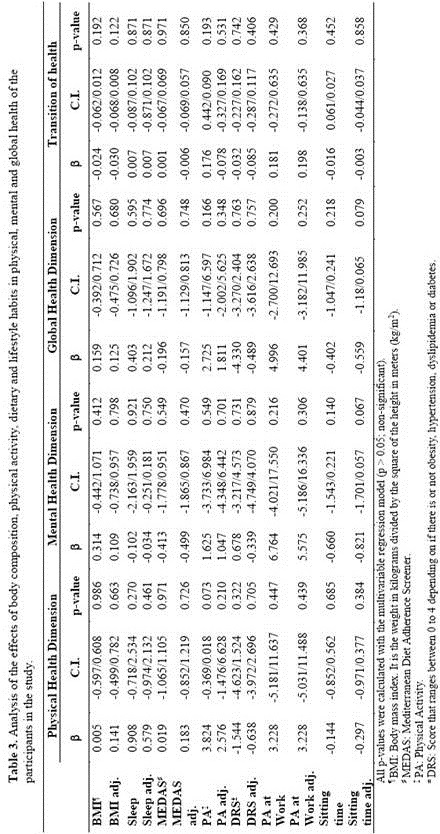
The average values of the three dimensions and the transition of health question of the population analyzed were not significantly influenced by any of the items analyzed. However, it had been found that physical activity had a marginal effect on physical health dimension, just as sitting time adjusted by sex and age is marginally significant for mental health dimension and global health dimension, which means that the minutes of physical activity tends to improve health (Table 3).
Discussion
Health is a concept that has great importance worldwide for the entire population and theere are multiple factors that influence on it. In 1974, Marc Lalonde, distinguished four main groups of factors that influence health: Health care organizatin, factors biolognetic, living enviroment and lifestyle(14). For WHO, quality of life related to health emphsized the consequesnces on people, who have diseases and their treaatments, taking into account the perception of the patient and their capacity to live an useful and full life(15).
There are some studies that demonstrate the negative relationship between waist circumference and BMI with quality of life(16). In our study, this clear between BMI and quality of life variables has not been seen.
No association has been found between physical activity and quality of life, which is not consistent with other studies that show a direct association between physical activity and quality of life(17) and mental health(18). There was also no association with the consumption of alcohol and tobacco on quality of life, as expected, as found in the literature(19, 20).
The mean score obtained in some dimensions of the SF-36 questionnaire has been influenced by the age and sex of the participants, so that, in general, women have a worse quality of life than men and the elderly worse than young people. Stephen et al. (2001)(21), already found this relationship with all the domains of the questionnaire. However, for Muller et al. (2004)(22), there was no significant interaction between the SF-36 scores and either age or sex.
The results presented in this study indicate a marginal significant relationship between total physical activity minutes and physical health dimension of SF-36 questionnaire. These findings are consistent with the study of Päivärinne et al. (2018)(23), which describes a strong positive association between physical activity and health related quality of life, and also with the study of Bize et al. (2007)(24), in which a consistent association between both variables is observed. In this study, the sedentary lifestyle (daily sitting time) resulted in a reduction in the quality of life. In the research of Barcones-Molero et al. (2018)(25), a relation between physical inactivity and the prevalence of obesity was also observed, and therefore a decrease in the quality of life related to health.
Strengths and weakness
The main strength of the present pilot study is that the questionnaires have been designed and evaluated by the same research who has subsequently administered it and included the data in the database, which reduces bias due to misinterpretation of the questions or confusion.
Our study has some limitations. First, the generalizability of our findings (mostly no stadistically significant) is limited because all the study participants were healthy people and selected based on interest and values, whether the results can be generalized to persons at lower risk on to other settings requires further research. Second, since the SF-36, some of the diseases, physical activity and dietary habits were based on self reported measures, it is possible that a reporting bias could arise. Third, there may be a social desirability bias which participants may tend to answer the most socially accepted, such a greater practice of physical activity. Fourth, the sample size of the study no allowed research conclusion because is small, and therefore its statistical power is also small. To make the estimates more accurate, an increase in the sample size is required, and to avoid making type I (α-risk) or type II (β-risk) errors.
Acknowledgements
The authors thank to University of Navarra for the opportunity provided to carry out the study and all the staff members involved in the study.
Contributors
JA.M., M.C, S.N-C and B.C. designed the study. A.F.-M and B.C. conducted the initial analysis. S. N-C. and B.C. completed the analysis and drafted the paper. JA. M. and S. N-C commented on the draft paper. All authors read and approved the final manuscript.
Funding
Se reconoce con gratitud el apoyo científico de CIBERON del Instituto Carlos III de Madrid y NUTRITIPOS “Diseño y desarrollo de un sistema de identificación de nutritipos para un consejo nutricional precisión” de Gobierno de Navarra.
Competing interest
None declared.
Referencias
- Martínez González MA, Alonso Á, Bes-Rastrollo M, Alegre Garrido F. Conceptos de salud pública y estrategias preventivas : un manual para ciencias de la salud. Barcelona : Elsevier España, S.L.; 2013
- Organización Mundial de la Salud. Constitución de la Organización Mundial de la Salud. Doc básicos [Internet]. 2006;Suplemento:20. Available from: http://www.who.int/governance/eb/who_constitution_sp.pdf
- Gisbert JP, Calvet X, Ferrándiz J et al. Manejo del paciente con dispepsia. Guía de práctica clínica. Atención Primaria. 2012;44(12):728-33.
- World HEalth Organization. Helath Education Unit. Life-styles and health. Soc. Sci. Med. (Great Bretain). 1986; 22 (2):117-24.
- Comission of Social Determinants of Health. Closing the gap in a generation. World Health Organization [Internet]. 2008;246. Available from: http://www.who.int/social_determinants/final_report/csdh_finalreport_2008.pdf
- Gavidia Catalán V, Talavera M. La construcción del concepto de salud. Didáctica las Ciencias Exp y Soc [Internet]. 2012;0(26):161-75. Available from: http://ojs.uv.es/index.php/dces/article/view/1935
- Alonso J. La Medida de la Calidad de Vida Relacionada con la Salud en la Investigación y la Práctica Clínica. Gac Sanit [Internet]. 2000;14(2):163-7. Available from: https://www.sciencedirect.com/science/article/pii/S0213911100714506?via%3Di hub
8. Ruiz M, Pardo A. Calidad de vida relacionada con la salud: definición y utilización en la práctica médica. PharmacoEconomics Spanish Res Artic [Internet]. 2014;2(1):31-43. Available from: http://link.springer.com/10.1007/BF03320897
9. Badía X, Alonso J. La medida de la salud. Guía de escalas de medición en español. 4a edición. Unión Editorial, editor. Barcelona; 2007.
10. Vilagut G, Valderas JM, Montserrat F. Interpretación de los cuestionarios de salud SF 36 y SF 12 en España: Componentes físico y mental. Med Clin. 2008;130(19):726-35.
- Obidoa C, Reisine S, Cherniack M. How Does the SF 36 Perform in Healthy Populations? A Structured Review of Longitudinal Studies. J Soc Behav Heal Sci [Internet]. 2010;4(1):30-48. Available from: https://www.researchgate.net/publication/228706259_How_Does_the_SF-36_Perform_in_Healthy_Populations_A_Structured_Review_of_Longitudinal_St udies
- WHO. Global Physical Activity Questionnaire [Internet]. 2014;1-22. Available from:http://www.who.int/ncds/surveillance/steps/resources/GPAQ_Analysis_Gui de.pdf
- Hebestreit K, Yahiaoui-Doktor M, Engel C, Vetter W, Siniatchkin M, Erickson N, et al. Validation of the German version of the Mediterranean Diet Adherence Screener (MEDAS) questionnaire. BMC Cancer. 2017;17(1):1-10.
- Lalonde M. A new perspective on the health of canadians. Minist Natl Heal Welf. 1981;76.
- García H, Vera C, Lugo L. Calidad de vida relacionada con la salud en Medellín y su área metropolitana, con aplicación del SF-36. Rev Fac Nac Salud. 2014;32(1):26-39.
- Han TS, Tijhuis MAR, Lean MEJ, et al. Quality of life in relation to overweight and body fat distribution. Am J Public Health. 1998;88(12):1814-20.
- Sanchez-Villegas A, Ara I, Martínez-González MA, et al. Physical activity during leisure time and quality of life in a Spanish cohort: SUN (Seguimiento Universidad de Navarra) Project. Br J Sports Med. 2012;46(6):443-8.
- De La Cruz-Sánchez E, Moreno-Contreras MI, Pino-Ortega J, et al. Actividad física durante el tiempo libre y su relación con algunos indicadores de salud mental Actividad física durante el tiempo libre y su relación con algunos indicadores de salud mental en España. Salud Mental. 2011;4534(1):45-52.
- Guitérrez-Bedmar M, Bes-Rastrollo M, Martínez-Gonzalez MA. et al. Smoking status, Changes in smoking status and health-related quality of life: Findings from the SUN (“Seguimiento universidad de Navarra”) cohort. Int J Environ Res Public Health. 2009;6(1):310-20.
- Herrold AA, Pape TL-B, Li X, et al. Association Between Alcohol Craving and Health-Related Quality of Life Among Veterans With Co-occurring Conditions. Mil Med [Internet]. 2017;182(7):e1712-7. Available from: http://militarymedicine.amsus.org/doi/10.7205/MILMED-D-16-00360
- Walters SJ, Munro JF, Brazier JE. Using the SF-36 with older adults: A cross-sectional community-based survey. Age Ageing. 2001;30(4):337-43.
- Muller-Nordhorn J. Comparison of the short form (SF)-12 health status instrument with the SF-36 in patients with coronary heart disease. Heart [Internet]. 2004;90(5):523-7. Available from: http://heart.bmj.com/cgi/doi/10.1136/hrt.2003.013995
- Päivärinne V, Kautiainen H, Heinonen A, Kiviranta I. Relations between subdomains of physical activity, sedentary lifestyle, and quality of life in young adult men. Scand J Med Sci Sports [Internet]. 2018 Apr 1 [cited 2018 Aug 6];28(4):1389-96. Available from: http://doi.wiley.com/10.1111/sms.13003
- Bize R, Johnson JA, Plotnikoff RC. Physical activity level and health-related quality of life in the general adult population: A systematic review. Prev Med (Baltim). 2007;45(6):401-15.
25. Barcones-Molero MF, Sánchez-Villegas A, Martínez-González MA, et al. The influence of obesity and weight gain on quality of life according to the SF-36 for individuals of the dynamic follow-up cohort of the University of Navarra. Rev Clin Esp. 2018;218 (8):408-416.